
Learning, Behavioural or Sensory Challenges: Taylor & Trott Pyramid of Learning
When working with children (or clients of any age) who present with learning, behavioural or sensory challenges, we often face the question: Where do we begin? The Taylor & Trott Pyramid of Learning (1991) offers a conceptual framework to answer precisely that.
Kathleen Taylor (an occupational therapist) and Maryann Trott (a special educator) developed the Pyramid of Learning in 1991, drawing on the ideas of Jean Ayres and the sensory integration framework. While the Pyramid is widely reproduced in the occupational therapy and special education communities, its original formulation is less often directly cited; many modern sources present it as “adopted into” works such as How Does Your Engine Run? by Williams & Shellenberger (1996) .
The purpose of the Pyramid is to visually illustrate a “bottom-up” developmental hierarchy: foundational physiological and sensory systems support increasingly complex sensorimotor, perceptual, and cognitive functions. When there are deficits at a lower tier, the higher levels suffer. In our therapy model, we assess and remediate “lower level” roadblocks (e.g. sensory processing, reflex integration) before expecting changes in higher-order skills like attention, academic learning or behavior.
In more recent literature, the Pyramid has been framed as a “developmental hierarchy for sensory structures” it remains a conceptual scaffold (rather than a tightly validated clinical tool) but has strong heuristic and explanatory value in developmental and sensory-based therapies.
Our therapy programs: reflex integration works at foundational neural levels, and that aligns with the lower tiers of the Pyramid, thus enabling “flow-up” effects toward higher tiers (e.g. behaviour, learning, daily living).
Below I describe each tier of the Pyramid (from base to apex) and discuss how reflex integration and other tailored developmental therapies can operate in each level, and how addressing each level can reduce impediments in clients’ presenting profiles.
The Tiers of the Taylor & Trott Pyramid of Learning
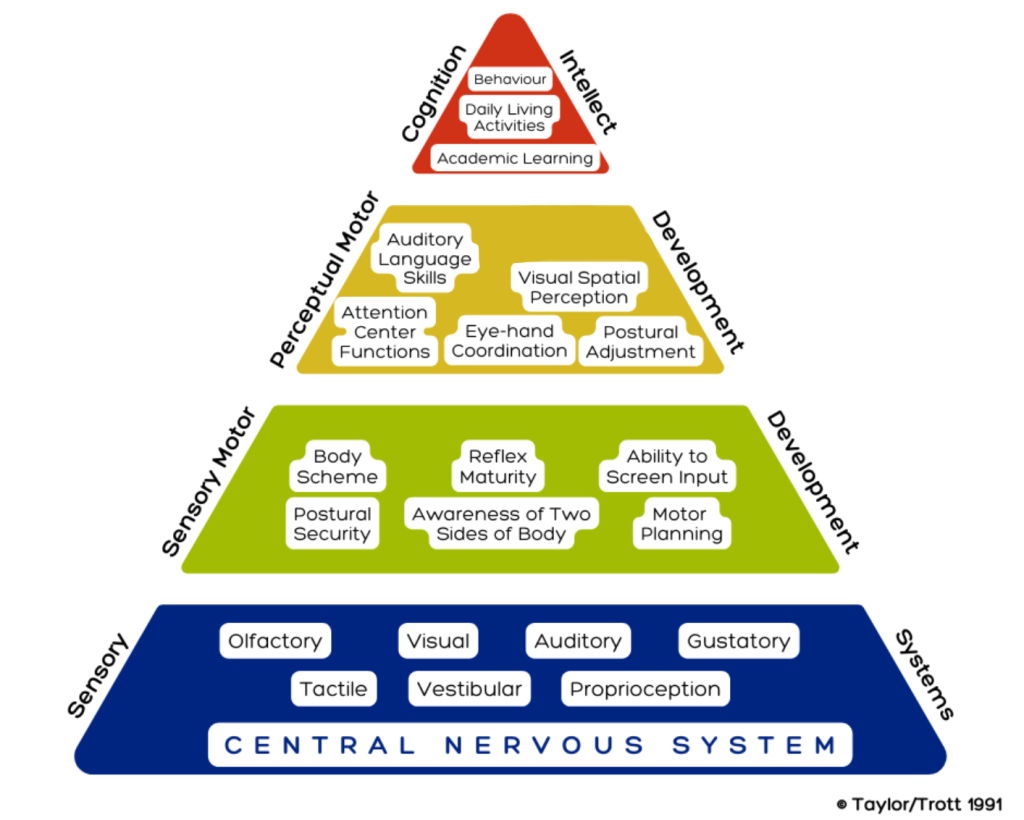
The Pyramid is typically depicted in five levels. From bottom (foundation) to top, they are:
- Central
- Nervous System (CNS)
- Sensory Systems
- Sensory Motor Development
- Perceptual Motor Development
- Cognition / Intellect / Functional Skills
Below is an expanded explanation of each, how they relate to reflex integration, and how therapeutic intervention may proceed.

