
Thumb Sucking, Dummy Use, and Fussy Eating: What Your Child’s Nervous System Is Actually Telling You
You have probably been told it is just a habit. Or that they will grow out of it. Or, and this one stings, that you just need to be firmer about it.
If your child is still sucking their thumb or dummy well beyond toddlerhood, or refuses most foods based on texture, smell, or appearance, the advice you have likely received has focused on the behaviour itself. Take the dummy away. Offer the food repeatedly. Use a reward chart.
But what if the behaviour is not the problem? What if it is the solution, your child’s nervous system doing exactly what it needs to do to feel regulated and safe?
At Tailored Developmental Therapies, we see these patterns regularly. And almost always, there is a neurological explanation that makes complete sense once you understand it, and that points toward a very different kind of support than behaviour management.
Does this sound like your child? Our free 30-minute phone consultation is a great first step, we can help you make sense of what you are observing and whether TDT’s programs are the right fit. Book your complimentary call, available Mondays 3:30–4:30pm.
These Are Not Habits. They Are Regulatory Strategies.
Every behaviour a child repeats has a purpose, even when that purpose is not immediately obvious to the adults around them.
Thumb and dummy sucking, oral seeking, and food avoidance are almost always subconscious strategies the nervous system has found to manage overwhelming or under-stimulating sensory experiences. They are not naughtiness. They are not manipulation. They are a child’s best available answer to a question their nervous system is asking constantly: Am I safe? Am I regulated? Do I know where my body is?
Understanding this shifts everything. Instead of trying to stop the behaviour, which often increases anxiety and makes the underlying need more acute, we can ask what the behaviour is communicating and address that need at its source.
This is the same principle that underpins our approach to demand avoidance, sensory seeking through heavy work, and the nervous system regulation work that sits at the foundation of everything we do at TDT.
Thumb Sucking and Dummy Use: The Nervous System Connection
The sucking action is one of the most powerful self-regulation tools a human nervous system has access to, and it is available from birth. This is not a coincidence. The oral region is extraordinarily rich in sensory nerve endings, and the act of sucking stimulates two major regulatory pathways: the trigeminal nerve and the vagus nerve.
When a child presses their thumb against the roof of their mouth, they are directly stimulating the trigeminal nerve — the largest cranial nerve in the face — which has a measurable calming effect on the nervous system. They are also activating the vagus nerve, which regulates heart rate, breathing, digestion, emotional state, and the capacity for social engagement. In other words, they have discovered, completely intuitively, one of the most effective regulation tools available to them.
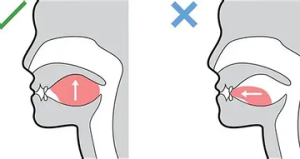
Tongue Posture Diagram
The question is not why are they doing this, the answer to that is clear. The question is why does their nervous system need this level of calming input to feel regulated, and what can we do about that underlying need.
The Role of Retained Oral Reflexes
In early infancy, the sucking and rooting reflexes are essential. They ensure a baby can latch, feed, and survive. As the brain matures, these reflexes are designed to integrate, to be absorbed into the more voluntary, sophisticated oral movements needed for speech, chewing, and swallowing.
When they do not integrate as expected, the nervous system may continue to rely on primitive sucking patterns as a default regulatory strategy. The thumb or dummy becomes the most accessible version of the input the retained reflex is seeking.
Retained oral reflexes can also affect speech and communication development in ways that are not always immediately obvious, contributing to unclear articulation, difficulty with sound sequencing, jaw instability, or tongue thrust. This is why we often see thumb sucking and speech difficulties appearing together in the same child, and why addressing the underlying reflex pattern can produce improvements in both areas simultaneously.
The Impact on Oral Development
Prolonged thumb or dummy use is not simply a developmental curiosity, it can have real physical consequences for oral structure. Consistent pressure on the roof of the mouth affects palate development, tongue resting position, and dental alignment. It can contribute to a high-arched palate, which in turn affects breathing patterns, as the palate forms the floor of the nasal cavity.
This is why the goal of our work is not to simply remove the thumb or dummy, which the child will resist because they genuinely need the regulatory input, but to address the underlying nervous system need so the child no longer requires the behaviour to feel regulated. When that happens, the behaviour reduces or stops naturally, without distress.
You might recognise this in your child: needs to suck or chew to settle, returns immediately to thumb or dummy when anxious or tired, has open-mouth resting posture, snores or mouth breathes at night, has been slow to develop clear speech.
The Breathing Connection
Oral posture and breathing patterns are deeply connected, and both connect directly to nervous system regulation.
When a child habitually breathes through their mouth rather than their nose, which is common in children with retained oral reflexes, high-arched palates, or chronic congestion, several regulatory systems are affected. Nasal breathing warms, filters, and humidifies air before it reaches the lungs, and it produces nitric oxide, which supports oxygen delivery and immune function. Mouth breathing bypasses all of this.
Perhaps more significantly, chronic mouth breathing tends to maintain a pattern of shallow, chest-based breathing, which keeps the nervous system in a mild state of activation, the opposite of the calm, regulated state we are trying to support. This creates a cycle: the child mouths, breathes through their mouth, maintains shallow breathing, stays mildly activated, and reaches for the oral input again.
This is one of the reasons belly breathing and nasal breathing practices are a consistent part of TDT’s programs, and why we address oral posture as part of the broader picture rather than in isolation.
Encouraging your child to breathe through their nose, even briefly and playfully, can be a gentle starting point. Try ‘smell the flowers, blow out the candles’ as a simple game. Any progress here supports the vagus nerve, reduces baseline arousal, and makes it slightly easier for the nervous system to regulate without oral seeking. Read more in our post on the importance of belly breathing.
Fussy Eating and Sensory Defensiveness: What Is Really Going On
Fussy eating is one of the most common and most misunderstood challenges parents bring to us. It is also one of the most guilt-inducing, parents often wonder what they are doing wrong, whether they introduced foods incorrectly, or whether they have somehow caused the problem.
In the vast majority of cases, the answer is none of the above. Significant food avoidance based on texture, smell, appearance, or temperature is almost always a sensory defensiveness response, the child’s sensory system is registering certain food properties as genuinely threatening, and the avoidance is a protective response, not a choice.
Why the Sensory System Reads Certain Foods as Threatening
A child whose nervous system is already under strain from retained primitive reflexes, poor interoception, or dysregulated sensory processing has less capacity to tolerate novel or intense sensory input. The proprioceptive and tactile systems that should help the mouth confidently explore different textures may be over-reactive, sending exaggerated threat signals in response to ordinary food experiences.
This is why the fussy eater so often has a very specific and narrow set of “safe” foods, usually those with predictable, non-surprising textures and smells. Smooth, dry, uniform, or crunchy foods are most commonly tolerated because they do not produce unexpected sensory events in the mouth. Mixed textures, strong smells, soft or mushy foods, and anything that changes consistency when chewed are most commonly rejected.
Understanding this also helps explain why the standard advice, “just keep offering it, they will eventually accept it”, often does not work for these children. If the nervous system is reading broccoli as a genuine threat, repeated exposure to broccoli does not reduce the threat response. It may actually entrench it.
You might recognise this in your child: gags at the sight or smell of certain foods, cannot tolerate foods touching each other on the plate, will only eat from a very limited rotation of ‘safe’ foods, becomes distressed or rigid at mealtimes, takes an extremely long time to eat or refuses to eat in new environments.
The Connection to Retained Reflexes
Several primitive reflexes are directly relevant to oral sensory defensiveness and fussy eating. The Babkin reflex (which links hand pressure to mouth opening) and retained versions of the sucking, rooting, and gag reflexes can all contribute to exaggerated oral sensitivity and reduced tolerance for new textures.
When these reflexes integrate through targeted reflex integration work, the mouth’s sensory system typically becomes less defensive. Foods that previously triggered a strong rejection response become more tolerable, not because the child has been pushed or rewarded into eating them, but because the nervous system no longer reads them as a threat.
This is also why fussy eating so frequently appears alongside other sensory sensitivities, to clothing textures, haircuts, toothbrushing, or loud environments. These are all expressions of the same underlying sensory processing pattern, rooted in the same foundational nervous system organisation. You can read more about how these foundational issues connect in our post on the Taylor & Trott Pyramid of Learning.
Practical Strategies You Can Start at Home
These strategies are designed to gently support the nervous system, build oral confidence, and reduce the underlying need for regulatory oral seeking. They work best as part of a consistent daily routine rather than as occasional interventions.
1. Support Oral Exploration
The goal here is to make oral sensory exploration feel safe and pleasurable, not to force new foods or new textures. The nervous system learns through positive, low-pressure exposure over time.
- Offer sticky or textured foods such as peanut butter, soft fruit, or yoghurt in a playful, no-pressure context, not at mealtimes initially
- Encourage your child to run their tongue along their teeth and the roof of their mouth, make it a game
- Blowing through straws, blowing bubbles, or blowing up balloons strengthens oral muscles and stimulates the calming pathways of the vagus nerve
- Vibrating toothbrushes can help desensitise the mouth gently over time, start with the gums rather than the teeth if there is significant defensiveness
- Chew tubes or chew jewellery provide organised, predictable oral input that can reduce the need for thumb or clothing chewing

Child blowing bubbles
💡 Never force oral exploration, this will increase defensiveness, not reduce it. The principle is always safety first. If your child is willing to touch a new food but not put it in their mouth, that is meaningful progress and worth celebrating.
2. Support Calm Through Nasal Breathing
Nasal breathing activates the parasympathetic nervous system and directly supports the vagus nerve, the same pathway that thumb sucking is trying to access. Building gentle nasal breathing practice into the day gives the nervous system an alternative route to regulation.
- ‘Smell the flowers, blow out the candles, inhale slowly through the nose, exhale slowly through the mouth
- Triangle breathing or box breathing for older children, simple visual patterns make it engaging
- Humming and singing also stimulate the vagus nerve through the throat and are a natural regulation tool that many children use intuitively
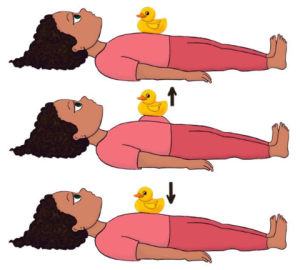
Diagram on how to Belly Breath
Read more about the full benefits of nasal breathing and diaphragmatic breathing in our post on the importance of belly breathing.
3. Encourage Gentle Head and Jaw Movement
Slow, gentle head movements and jaw exercises can help integrate the reflexes that contribute to oral defensiveness and thumb sucking. These do not need to be formal exercises, they can be woven into play naturally.
- Slow side-to-side head rolls, gentle and never forced
- Chin tucks, gently bringing the chin toward the chest and holding briefly
- Gentle jaw stretches, opening wide, moving side to side slowly
- Chewing resistive foods such as dried fruit, raw carrot, or bread crusts — if tolerated — provides proprioceptive input to the jaw joints
💡 If your child experiences dizziness with head movements, discontinue and mention this to your therapist. Dizziness during head movement can indicate a retained TLR or vestibular processing issue worth assessing.
4. Build Regulation Through the Body First
Oral seeking and food avoidance are often at their most intense when the whole nervous system is dysregulated. Addressing the body’s regulation needs before mealtimes or before oral exploration activities can make a significant difference.
Heavy work activities done 10–15 minutes before a mealtime can meaningfully reduce oral defensiveness by bringing the whole nervous system to a calmer baseline before food is introduced. For a full activity toolkit, see our post on heavy work activities that support nervous system regulation.
When to Seek Professional Support
Home strategies are a valuable starting point, but some presentations benefit from — or require — professional assessment and targeted therapeutic support.
Consider seeking professional support if your child:
- Has a very significantly restricted diet that is affecting their nutrition, growth, or social participation
- Has persistent thumb or dummy use that is affecting their dental development, speech clarity, or sleep
- Has suspected tongue tie or lip tie, these are structural issues that can affect oral posture, feeding, and speech and warrant assessment by a speech therapist or relevant specialist
- Has a high-arched palate, open-mouth resting posture, or persistent mouth breathing, these can affect airway function and warrant review
- Is showing significant distress around mealtimes or oral activities that is affecting family quality of life
- Has oral sensory challenges alongside other sensory sensitivities, learning difficulties, or behavioural concerns
At TDT, Fiona (our speech therapist) and Emily (our director) work collaboratively on cases where oral development, reflex integration, and communication intersect. For many families this joint approach — addressing the nervous system foundations alongside the speech and oral motor skills, produces faster and more sustainable progress than either approach alone.
Our speech therapy sessions use a DIR Floortime and play-based approach, which means therapy is led by the child’s interests and comfort, never forced or pressured. This is particularly important for children who have experienced distress around oral activities, as rebuilding safety and trust is always the first priority.
The Bigger Picture: Why These Behaviours Often Appear Together
One of the things we hear most from families is surprise at how connected these different behaviours are. A child who sucks their thumb is also a fussy eater. A child who refuses foods is also sensitive to clothing textures. A child with a limited diet also struggles with transitions, or gets overwhelmed easily in busy environments, or has sleep difficulties.
This is not a coincidence. These are all expressions of the same underlying pattern, a nervous system that is working very hard to manage sensory input and maintain regulation, using whatever tools it has available.
When we address the foundational nervous system organisation through reflex integration and neuroplasticity-based programs, families consistently report that multiple areas improve at once, not because we specifically targeted each one, but because we addressed the common root. Mealtimes become easier. The thumb or dummy is needed less. Sleep improves. Transitions become less distressing.
This is the power of working from the bottom up, the approach that sits at the heart of everything we do at TDT. If you have not yet read our post on the Taylor & Trott Pyramid of Learning and the bottom-up approach to development, it explains the full framework and why foundational nervous system work produces results across so many different areas of a child’s life.
You can also read about what families typically experience as that foundational work begins to take effect in our post on positive changes during therapy.
Frequently Asked Questions
At what age should I be concerned about thumb or dummy sucking?
Most developmental guidelines suggest that dummy use beyond 12 months and thumb sucking beyond 4–5 years can begin to affect dental development and oral posture. However, the more important question is not the age but the function, if the behaviour is serving a significant regulatory need, removing it without addressing that need is unlikely to be successful and may increase anxiety. If you are concerned, a conversation with our team is a good starting point regardless of age.
My child’s diet is so restricted it is affecting their nutrition. Is there something TDT can do?
Yes. Significantly restricted diets that affect nutrition and growth need professional support, home strategies alone are not sufficient in these cases. Fiona’s speech therapy sessions and Emily’s reflex integration programs can both contribute to expanding food tolerance, and we work collaboratively to address the oral sensory and neurological foundations together. Please book a phone consultation so we can discuss the picture in full.
Can these issues be supported through NDIS?
Yes. TDT works with NDIS participants, and our speech therapy and therapeutic programs may be accessible under relevant NDIS support categories for plan-managed and self-managed participants. We are happy to discuss this during your complimentary phone call.
Is this connected to my child’s speech difficulties?
Very often, yes. Retained oral reflexes, oral sensory defensiveness, and mouth breathing patterns all have direct implications for speech and communication development. The oral motor skills needed for clear speech rely on the same foundational integration that influences thumb sucking and food acceptance. This is one of the reasons TDT’s approach, addressing both the nervous system foundations and the speech skills together tends to produce more comprehensive progress than targeting speech alone.
We have tried everything. How is TDT different?
The most common reason that behavioural approaches to thumb sucking and fussy eating do not produce lasting results is that they target the behaviour without addressing the nervous system need that is driving it. TDT’s programs work at the foundational level, reflex integration, nervous system regulation, oral motor development, which means that when change happens, it tends to be genuine and lasting rather than dependent on ongoing management. Our free phone consultation is the best place to explore whether our approach is the right fit for your family.
Is your child’s nervous system asking for something different?
Book your free 30-minute phone consultation with the TDT team.
Emily and Fiona work together to address the oral, sensory, and nervous system foundations.



