
How We Learn: TDT’s Assessment Process and How We Find the Right Starting Point for Your Child
When a family first contacts Tailored Developmental Therapies, one of the most common questions we hear is: “Where do we even begin?”
It is a genuinely good question. Learning difficulties, behavioural challenges, sensory sensitivities, speech delays, emotional dysregulation, coordination difficulties, these are the things families can see. What they often cannot see is the underlying developmental picture that is producing them. And without understanding that picture clearly, it is very easy to target the visible symptoms while the root causes go unaddressed.
At TDT, we begin with assessment. Not with a standard checklist or a brief intake form, but with a comprehensive, individualised evaluation of where a client sits within the Taylor & Trott Pyramid of Learning, the developmental framework that guides everything we do. This assessment tells us where the foundational work needs to happen, and it is the basis on which every TDT program is built.
This post explains the Pyramid framework, what our assessment covers, what we are looking for, and what happens after assessment, so that families considering TDT have a clear picture of what the journey looks like before they take the first step.
Curious about what TDT’s assessment process looks like for your child’s specific situation? Our free 30-minute phone consultation is the right starting point, we will listen carefully and help you understand whether TDT is the right fit. Book your complimentary call — available Mondays 3:30–4:30pm.
The Framework Behind Our Approach: The Taylor & Trott Pyramid of Learning
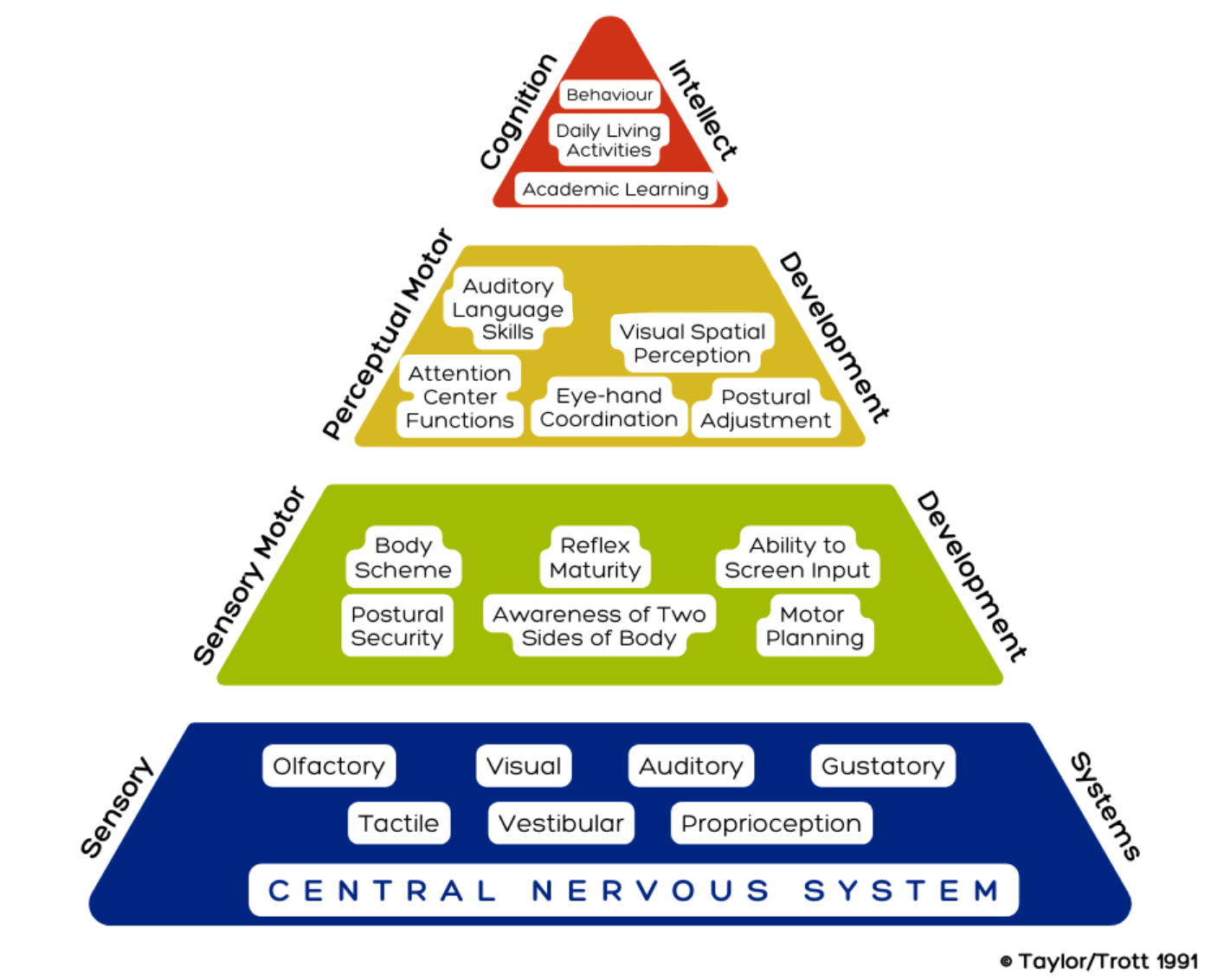
The Taylor & Trott Pyramid of Learning (1991) is the conceptual framework at the heart of TDT’s clinical approach. Developed by occupational therapist Kathleen Taylor and special educator Maryann Trott, it maps the developmental hierarchy of the brain and nervous system, showing that complex skills like learning, behaviour, and emotional regulation depend on simpler foundational systems being organised and functional first.
The Pyramid has five levels, from the base to the apex:
Level 1: Central Nervous System: the foundation, brain and spinal cord, autonomic regulation, arousal systems, neural connectivity, and the integration of primitive reflexes. If this level is disorganised, everything above it is affected.
Level 2: Sensory Systems: the body’s input channels, tactile, proprioceptive, vestibular, visual, auditory, interoceptive. These systems deliver the raw data the brain needs to make sense of the world.
Level 3: Sensory Motor Development: the integration of sensory input with motor output, postural stability, bilateral coordination, body awareness, motor planning, and reflex maturity.
Level 4: Perceptual Motor Development: where perception and action meet in refined ways, eye-hand coordination, visual-spatial processing, auditory language skills, attention, and ocular motor control.
Level 5: Cognition, Learning, and Functional Skills: the apex, academic learning, behaviour, emotional regulation, executive function, social skills, and independence in daily life. This is the level families most often notice. But it depends on all four levels beneath it being solid.
The Pyramid’s central insight is straightforward but profound: you cannot reliably build skills at the top if the foundation is unstable. Trying to address learning difficulties, behaviour problems, or emotional regulation challenges without first understanding and addressing what is happening in the foundational levels is like trying to build a roof without walls.
This is why TDT does not begin with the presenting problem. We begin with the foundation.
For a full explanation of the Pyramid and what each level means for your child’s development, read our dedicated post: Why Your Child Struggles to Learn or Behave: A Bottom-Up Approach to Therapy.
What Can Disrupt the Foundation and Why It Matters
Many things can affect the development of the lower Pyramid levels, and many of them happen before families are even aware anything is different about their child’s development.
Factors that can affect foundational development include:
- Limited physical activity by the mother during pregnancy, which affects the baby’s vestibular and sensory development in utero
- Difficult labour and birth, particularly births involving interventions such as forceps, ventouse, or emergency caesarean, which can affect early reflex integration
- Prematurity, which shortens the in-utero developmental period during which foundational neural connections are being laid down
- Limited tummy time in early infancy, which is one of the primary ways the brain integrates early primitive reflexes and builds the sensory motor foundation
- Skipping developmental milestones such as crawling, which provides critical bilateral integration and vestibular development
- Significant early illness or hospitalisation
- Genetics, some developmental patterns are heritable
- Diet and nutrition during critical developmental periods
When any of the lower Pyramid levels are less than optimally developed, the root cause will almost always be found in the central nervous system and sensory system, Levels 1 and 2. And the presenting difficulties that families seek help for — at Level 5 — are almost always the downstream consequences of something happening much further down.
💡 This is why TDT only offers programs where there are genuine behaviour or learning difficulties evident. We are not a general enrichment service. We are a targeted, assessment-driven practice that identifies specific foundational difficulties and addresses them directly.
What TDT’s Assessment Actually Covers
TDT’s comprehensive assessment is not a standard checklist. It is an individualised evaluation that looks at multiple layers of a client’s developmental picture, using a combination of standardised tools, clinical observation, and family and school history. The goal is to build a complete map of where the foundational difficulties are, not just what the presenting problems look like.
Assessment at TDT typically covers:
🧠 Reflex Integration: Emily assesses the presence and degree of retained primitive reflexes, particularly those most commonly associated with learning, behaviour, sensory, and coordination difficulties. This includes the Moro reflex, Tonic Labyrinthine Reflex (TLR), Symmetrical and Asymmetrical Tonic Neck Reflexes (STNR/ATNR), Spinal Galant, Palmar, and others relevant to the client’s presenting profile.
👁️ Visual Processing: TDT tests eight specific areas of visual processing: visual discrimination, visual memory, spatial relationships, form constancy, sequential memory, figure-ground perception, visual closure, and visual stress. These are the areas that standard optometric testing does not cover, and weaknesses here are among the most common and most commonly missed contributors to reading and learning difficulties. Read more in our post on
visual stress and visual processing difficulties.
👂 Auditory Processing: Assessment of how the brain processes what it hears, including discrimination of speech sounds, auditory memory, and the ability to process language in the presence of background noise. Auditory processing difficulties are a significant contributor to language and learning difficulties and are frequently unidentified.
🖊️ Fine Motor and Gross Motor Skills: Assessment of coordination, bilateral integration, motor planning (praxis), postural stability, and the quality of movement at both the fine and gross motor level. The Goodenough Draw-A-Person test is one of the key tools TDT uses here, see link below.
Goodenough Draw-A-Person test: a drawing task that reveals a remarkable amount about a child’s visual perception, executive function, working memory, fine motor control, and bilateral integration in a single, non-threatening activity.
🔢 Executive Function and Learning Skills: Assessment of working memory, attention, planning, organisation, task initiation, and cognitive flexibility, the higher-order skills that sit at the top of the Pyramid and that are most directly affected when the foundational levels are not well organised.
💬 Communication and Language: Where relevant — and often in collaboration with Fiona — assessment of expressive and receptive language, speech clarity, oral motor function, and the relational and regulatory foundations that communication depends on.
🌡️ Interoception and Sensory Regulation: Assessment of the client’s ability to detect and respond to internal body signals, hunger, fullness, the need for the bathroom, pain, and the early signals of emotional states before they reach overwhelm. Poor interoception is a significant contributor to toileting difficulties, emotional dysregulation, and meltdowns that appear to come without warning, see link below.
Toileting difficulties, emotional dysregulation, and meltdowns that appear to come without warning.
Assessment findings are discussed with families in full. Emily explains what she has found in plain language — not in clinical jargon — and the program built from the assessment is grounded in those specific findings rather than in a standard protocol.
The Leaking Bucket: Why Targeted Assessment Matters
One of the ways Emily explains TDT’s approach to new families is through a simple analogy: imagine the brain as a bucket. Information goes in at the top. If the bucket has holes in it, representing weaknesses at the foundational levels of the Pyramid, that information leaks out before it can be stored, processed, or used. No matter how much you pour in at the top, the bucket keeps losing it through the holes.
Standard educational and therapeutic approaches often focus on pouring more in, more reading practice, more tutoring, more behaviour strategies, more rewards. And these approaches have genuine value. But they do not plug the holes. The information still leaks.
TDT’s assessment finds the holes. And TDT’s programs plug them, by addressing the specific foundational weaknesses that are causing the information to leak in the first place. Once the holes are plugged, the same input that was previously being lost becomes accessible, storable, and usable.
This is why families so often report that progress with TDT feels qualitatively different from progress with other approaches, not incremental and strategy-dependent, but more like a system that has finally started working the way it was meant to.
What TDT Programs Look Like After Assessment
Once the assessment is complete and findings have been discussed with the family, Emily builds an individualised program specifically targeting the foundational areas identified. No two programs are identical, because no two clients have the same developmental picture.
TDT programs typically include:
Daily Home Practice
The most important component of any TDT program is the daily home practice, short, specific exercises done consistently by the client (or by the family with the client) between sessions. This is where the neural change actually happens. The brain lays down new pathways through consistent, repeated stimulation, not through occasional intensive input. A ten-minute daily program done consistently is far more effective than weekly sessions without home practice between them.
Emily designs home programs to be genuinely manageable within real family life, not something that requires an additional hour each evening, but something that can be woven into the existing routine of a morning or bedtime.
Regular Sessions With Emily
Sessions with Emily provide the structured reflex integration and neuroplasticity work that the home program supports. Frequency varies by client, some benefit from weekly sessions, others from fortnightly, and is reviewed regularly as the program progresses. Sessions are available at TDT’s Mawson Lakes clinic, via Zoom, or in the client’s home.

Speech Therapy With Fiona
For clients where communication development is part of the picture, Fiona’s speech therapy sessions run alongside Emily’s programs, and for many clients, Emily and Fiona offer joint sessions that address both the nervous system foundations and the communication skills simultaneously. This integrated approach is one of TDT’s most distinctive clinical offerings and produces outcomes that neither approach achieves as effectively alone.
Read more about the speech and reflex integration connection in our post on speech and communication development and the role of primitive reflex integration.
Mentored Support Workers
For clients receiving NDIS-funded support, TDT’s mentored support workers extend the therapeutic program into the home and community environment, implementing the specific strategies and exercises that Emily has designed for the client, under Emily’s ongoing supervision. This ensures that the work of therapy is not limited to clinic sessions but is reinforced consistently throughout the client’s daily life.
Collaboration With Schools and Other Professionals
TDT works collaboratively with schools, teachers, learning support coordinators, occupational therapists, paediatricians, and other professionals involved with a client. We are willing to attend school meetings, contribute to learning support plans, and communicate directly with other providers, because the most effective therapeutic outcomes happen when everyone around a child is aligned and working toward the same goals.
Regular Progress Reviews
Progress is tracked throughout the program and reviewed regularly with families. TDT does not operate on a set-and-forget basis, programs are adjusted as the client develops, goals are updated as foundational progress opens new possibilities, and families are kept informed of what is changing and why.
Read more about what families typically notice as progress builds in our post on positive changes as therapy progresses.
We Work With Your Existing Team
TDT does not work in isolation. One of Emily’s core commitments is to work collaboratively with the other therapists, educators, and professionals already supporting each client. Where another provider’s goals and TDT’s programs can be aligned, and they very often can, we actively seek that alignment.
We also work with families to help them understand their child’s profile in language that is genuinely useful in conversations with schools, other therapists, and funding bodies. Advocacy for our clients, in educational settings, with NDIS planners, and in other professional contexts, is part of what TDT offers, not a separate service.
How to Get Started With TDT
Every family’s journey with TDT begins with the same first step: a free 30-minute phone consultation.
This is not a sales call. It is a genuine clinical conversation, an opportunity for you to tell us about your child, ask your questions, and for us to understand your situation well enough to give you an honest answer about whether TDT’s approach is the right fit. We will tell you clearly if we do not think we can help, and where we can we will point you toward someone who can.
Complimentary consultations are available on Mondays between 3:30 and 4:30pm, and can be booked via our website. Following the consultation, if TDT is the right fit, a comprehensive assessment will be scheduled, and from there, the program is built.
Sessions are available at our Mawson Lakes clinic (Shop 1/11 Parkway, Mawson Lakes SA 5095), via Zoom, or in your home or school. We work with NDIS participants across plan-managed and self-managed plans. No referral or diagnosis is required to make contact.
TDT’s values, growth, fun, self-respect, service, success, compassion, authenticity, community, knowledge, kindness, safety, and trustworthiness, are the criteria against which every program and every client relationship is built. When a family’s goals align with these values, we are genuinely confident that the work we do together can produce meaningful, lasting change.
Frequently Asked Questions
Do I need a referral or diagnosis to start with TDT?
No. TDT does not require a formal referral or diagnosis. Families can contact us directly and begin with the complimentary phone consultation. Our assessment process looks at what is actually happening in the nervous system and the developmental picture, not at diagnostic paperwork. A diagnosis does strengthen some conversations (with schools and NDIS planners), and we can help families understand the value and process of seeking one where relevant.
How long does the assessment take?
A comprehensive TDT assessment typically takes one to two sessions, depending on the client’s age, profile, and how much history needs to be gathered. Assessment sessions are not rushed, we take the time to build a thorough picture. Results and program recommendations are discussed with families following the assessment, and programs begin once goals and logistics have been agreed.
How do I know if TDT is right for my child?
The best way to find out is the complimentary phone consultation. In that conversation, we will ask specific questions about your child’s developmental history, current difficulties, and what you are hoping to achieve. We will be honest about whether TDT’s approach is likely to be effective for your child’s specific profile, including if we think another provider or approach would be a better fit. You can also read our post on how to choose the right therapist and the five questions that matter for a framework to help you evaluate any provider.
Can TDT help if my child has already been through other therapies?
Yes, and in fact, many of the families who come to TDT have already been through other interventions that produced limited or inconsistent results. This is often because those interventions addressed the presenting difficulties without identifying or addressing the foundational developmental picture underneath them. TDT’s assessment frequently reveals things that previous assessments have not looked for, particularly retained primitive reflexes and visual processing difficulties, and builds programs accordingly.
What age groups does TDT work with?
TDT works with individuals of all ages, from toddlers to adults. The Pyramid of Learning applies across the lifespan, and the foundational nervous system work TDT does produces meaningful change regardless of age. Programs are adapted to suit the individual’s developmental stage, learning profile, and goals.
Is TDT a registered NDIS provider?
Yes. TDT works with NDIS participants across plan-managed and self-managed plans. Our therapeutic programs, including reflex integration, neuroplasticity, speech therapy, and mentored support, are accessible under relevant NDIS support categories. We are happy to discuss how your plan can support a TDT program during your complimentary phone consultation.
Ready to find out where your child is on the Pyramid, and what to do about it?
TDT’s comprehensive assessment gives you a clear picture and a clear path forward.
Book your free 30-minute phone consultation, available Mondays 3:30–4:30pm.



